
LASER photocoagulation is considered the mainstay of treatment in pre-threshold type 1 ROP (Retinopathy of Prematurity). (more…)
Blog
-

Ocular Tuberculosis Part 4 – Diagnosis & Treatment
Our Previous Blog Ocular Tuberculosis Part 3
Generally, tuberculosis is known to affect the pulmonary system, but in some cases, it can also affect other organs (extra-pulmonary) like eyes. Ocular tuberculosis or tuberculosis uveitis is a chronic infection caused by Mycobacterium tuberculosis. This infection can occur in or around the eye. It can occur with or without clinical evidence of pulmonary tuberculosis. In addition, it can affect any tissue of the eye, sometimes without any characteristic manifestation. Hence, establishing the diagnosis of ocular tuberculosis is a great challenge. However, prompt and accurate diagnosis and quick treatment can help save the patient’s vision.
What are the difficulties and what is the importance of an accurate diagnosis of ocular TB?
Ocular Tuberculosis is extremely challenging to diagnose for the following reasons:
- There is no uniform diagnostic criteria laid down
- Biopsy and molecular diagnosis from the eye lesions is a challenge because it is a paucibacillary (containing only few bacilli) disease.
- We still do not know whether it is a direct infection from bacteria or it is a hypersensitivity reaction to the bacterial antigen/protein.
- Eye TB has protean manifestations and it mimics many other diseases.
- There may or may not be any signs of systemic tuberculosis
However, getting the diagnosis right is very critical, especially in ocular tuberculosis because it has implications on treatment and final visual outcome for the patient. In the presence of an inaccurate diagnosis, inadvertent use of steroids or immunosuppressive agents, which are the most commonly used drugs for treatment of uveitis, may lead to reactivation of latent tuberculosis and can actually worsen the disease and prognosis for the patient. Moreover, an undetected active systemic TB may even be life-threatening if patient is treated with only steroids or systemic immunosuppression.
What are the diagnostic tests used for ocular TB?
Following is a brief description of the diagnostic tests we use and their rationale.
- Ocular Imaging: Depending on the primary site of involvement, following individual or combination of imaging techniques are used:
-
- External eye photography (Figure 1)
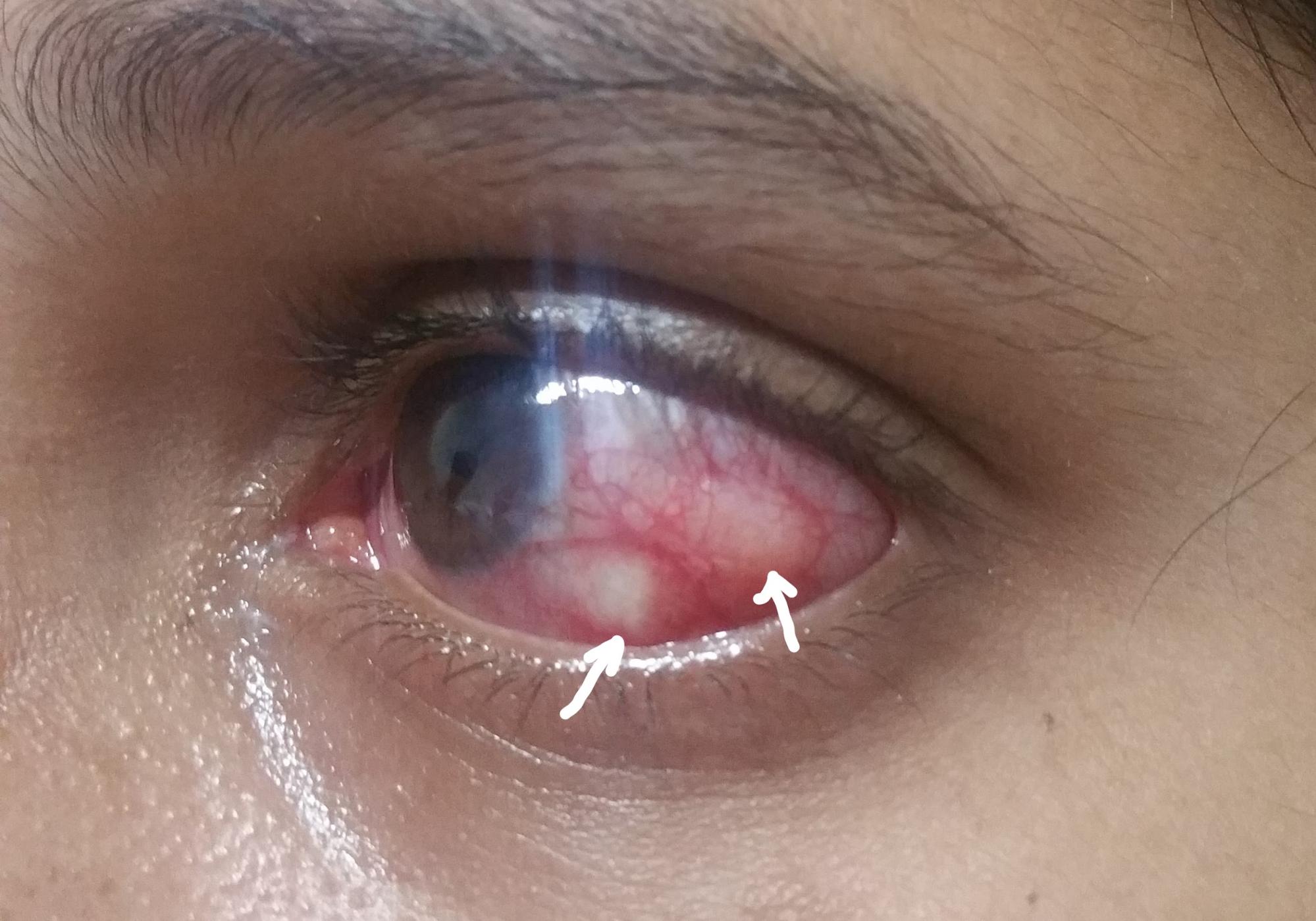
Figure 1. Left eye of a patient with multiple scleral nodules (arrows). - Fundus photography: a photograph of the retina (nerve layer at the back of the eye) (Figure 2)
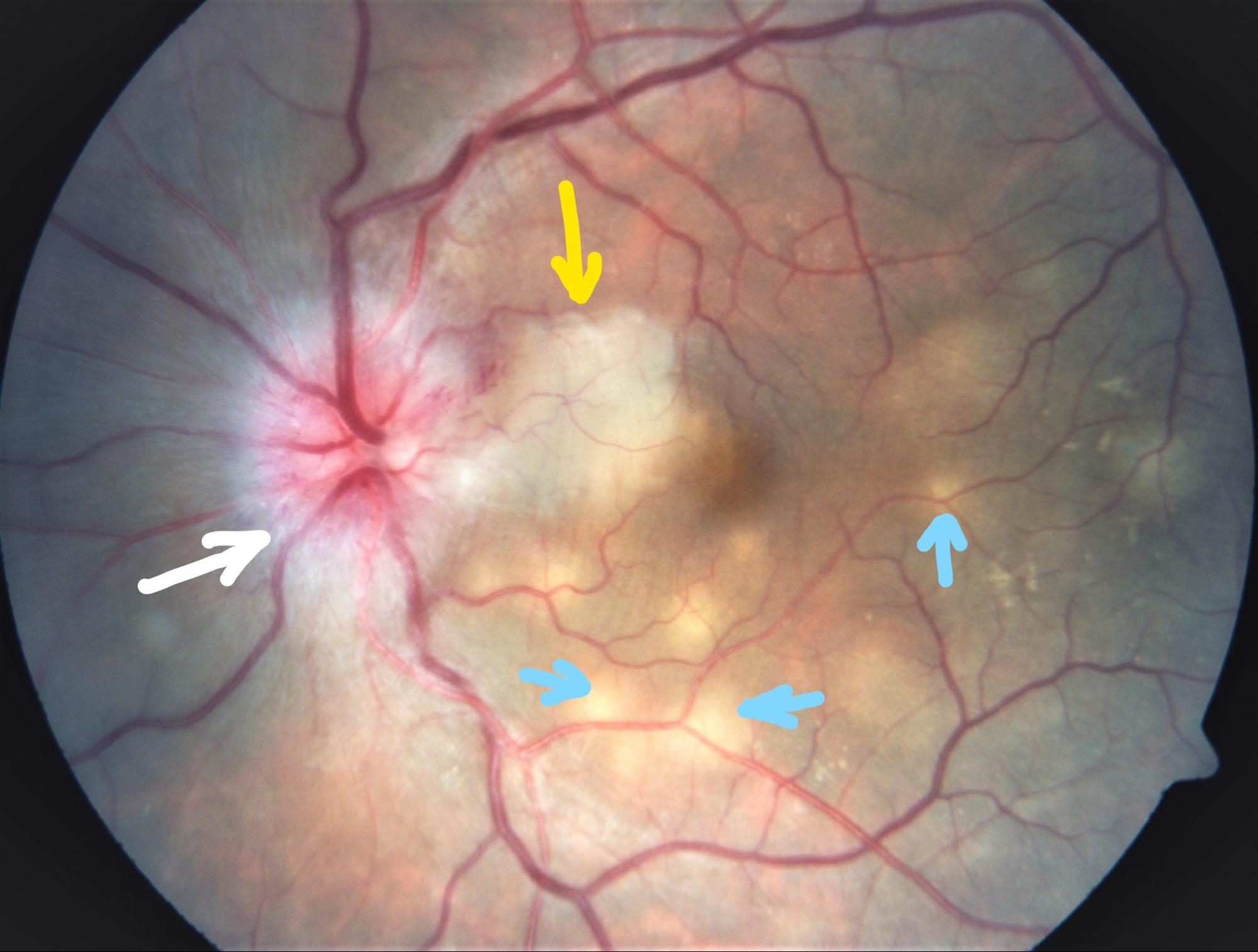
Figure 2. Fundus photograph of the left eye of a patient with optic disc swelling (white arrow) with whitening of adjacent retina (neuroretinitis, shown by yellow arrow)) and multiple deep yellow lesions (choroiditis, shown by blue arrows) - Fundus autofluorescence: photo of the retina using special filters where area of interest is the retinal pigment epithelium. (Figure 3).
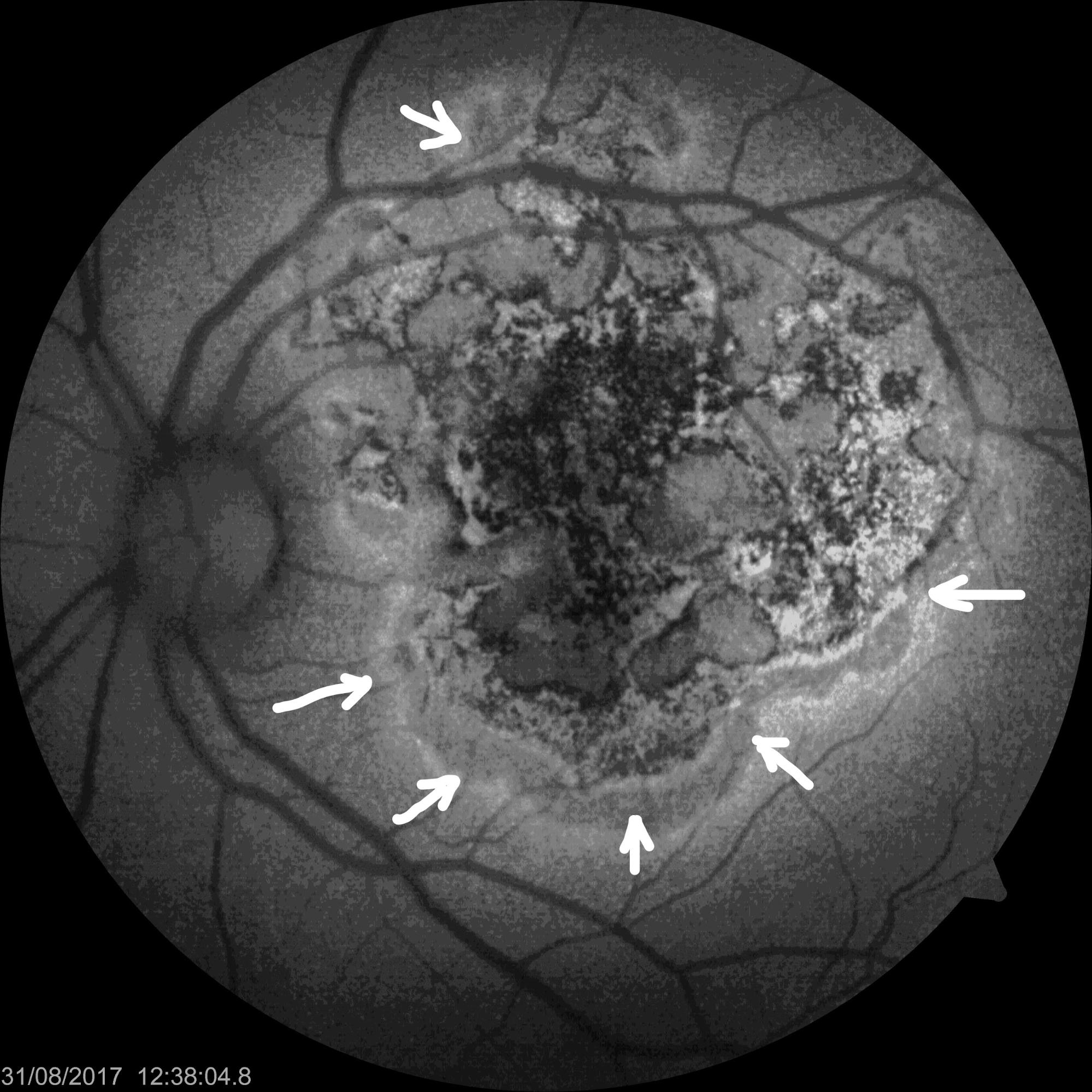
Figure 3. Fundus autofluorescence picture of a patient with left eye serpiginoid choroiditis (disease of the RPE and choroid, presumably due to tuberculosis). The lesions are active at the margins (arrows). - Fluorescein angiography: Where a fluorescein dye is injected in a vein of the forearm and its transit through the choroid, retina and retinal blood vessels is studied by photographs. (Figure 4)
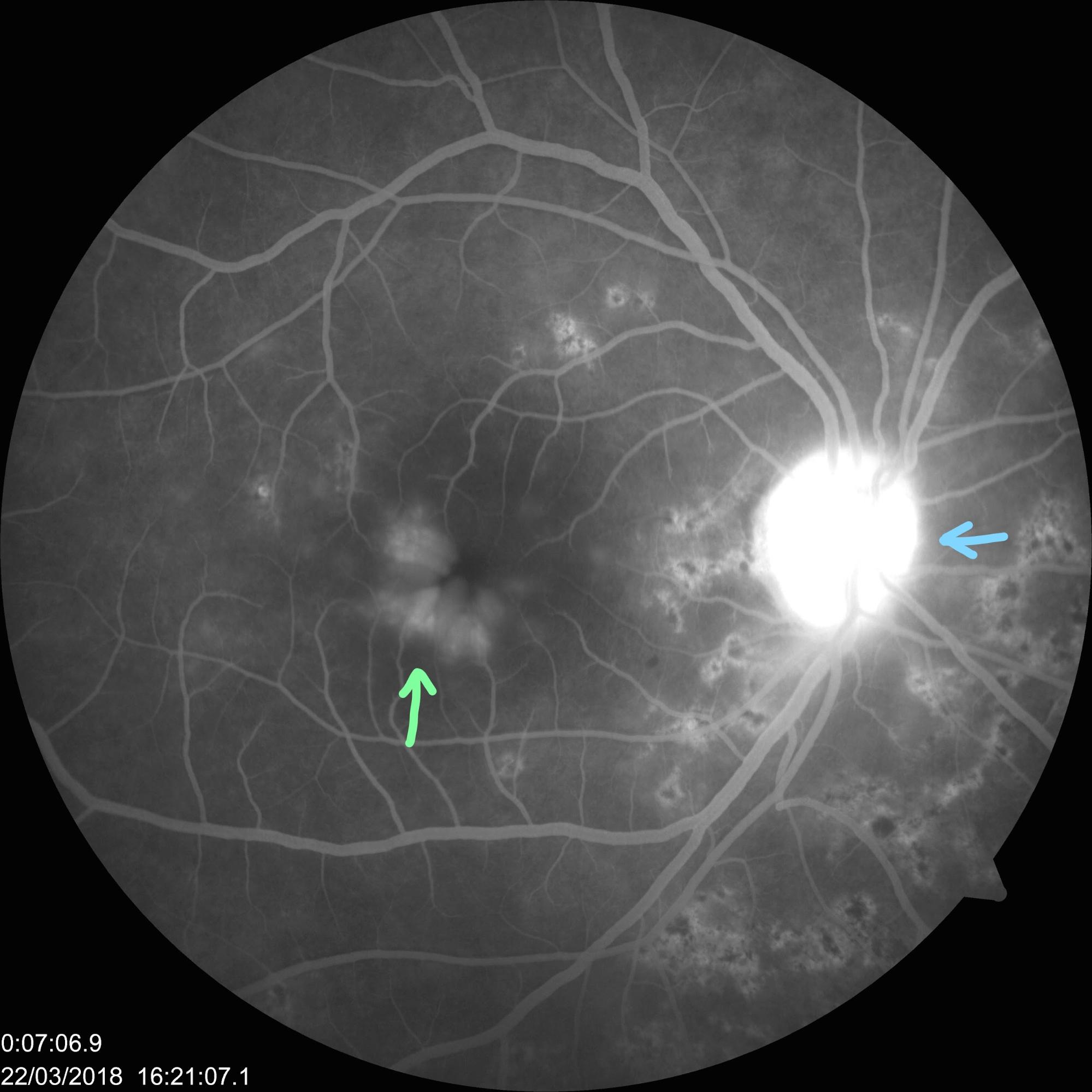
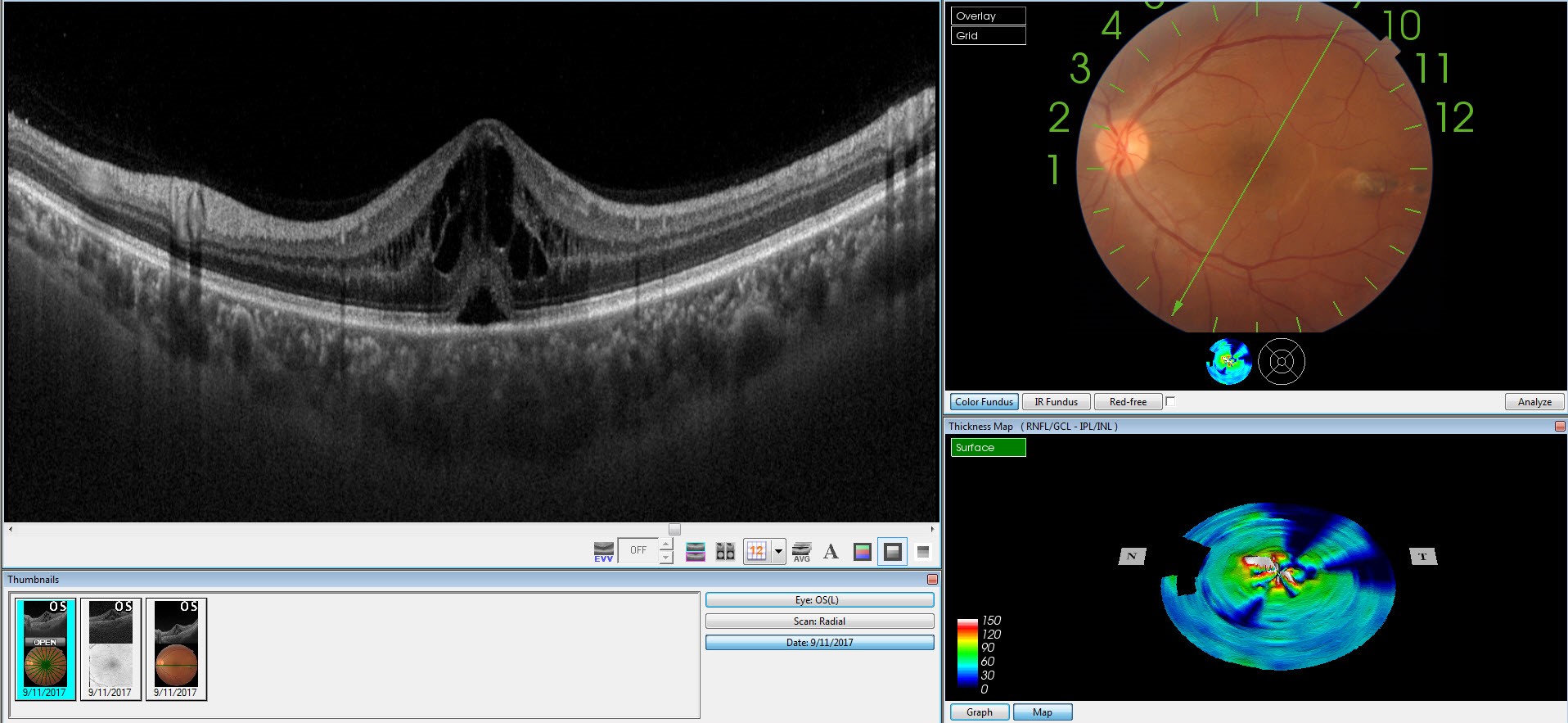
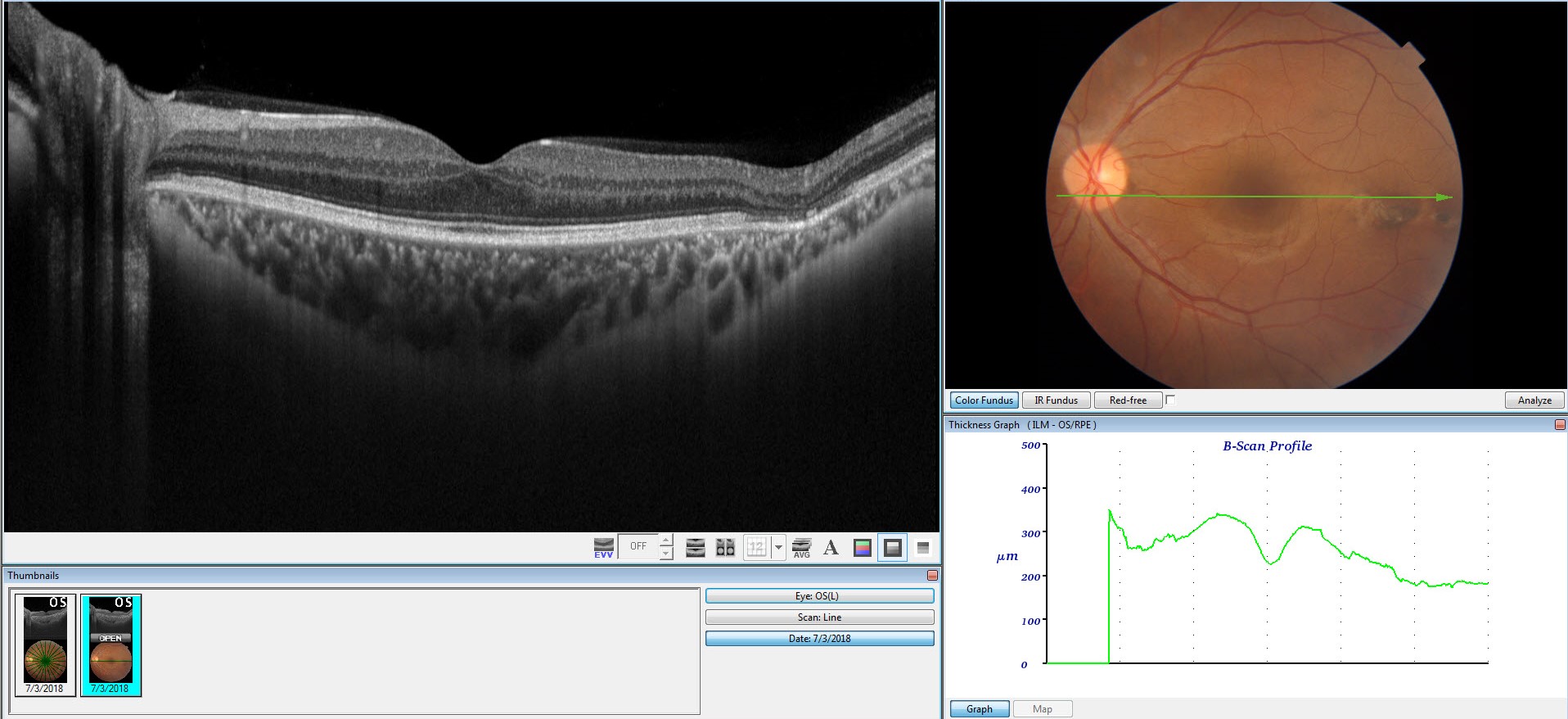
Figure 4. Fluorescein angiography picture of the right eye of a patient with posterior uveitis, showing a hot disc (bright signal at the optic nerve, shown by blue arrow)) and leakage at the macula (centre of the retina, shown by green arrow). - OCT: It is a non-invasive scanning method to study cross-section of the retina and choroid. It is particularly useful in studying the vitreo-retina interface, swelling/ fluid collection inside the retina (cystoid macular oedema) or under the retina (subretinal fluid), abnormality in various layers of the retina and choroid. (Figure 5)
Figure 5. OCT picture of a patient with cystoid macular oedema (swelling of the centre of the retina), showing fluid spaces and the different layers of the retina. - OCT angiography: This is a non-invasive, no dye, no injection angiography to study the deep retinal and choroidal vasculature. (Figure 6)
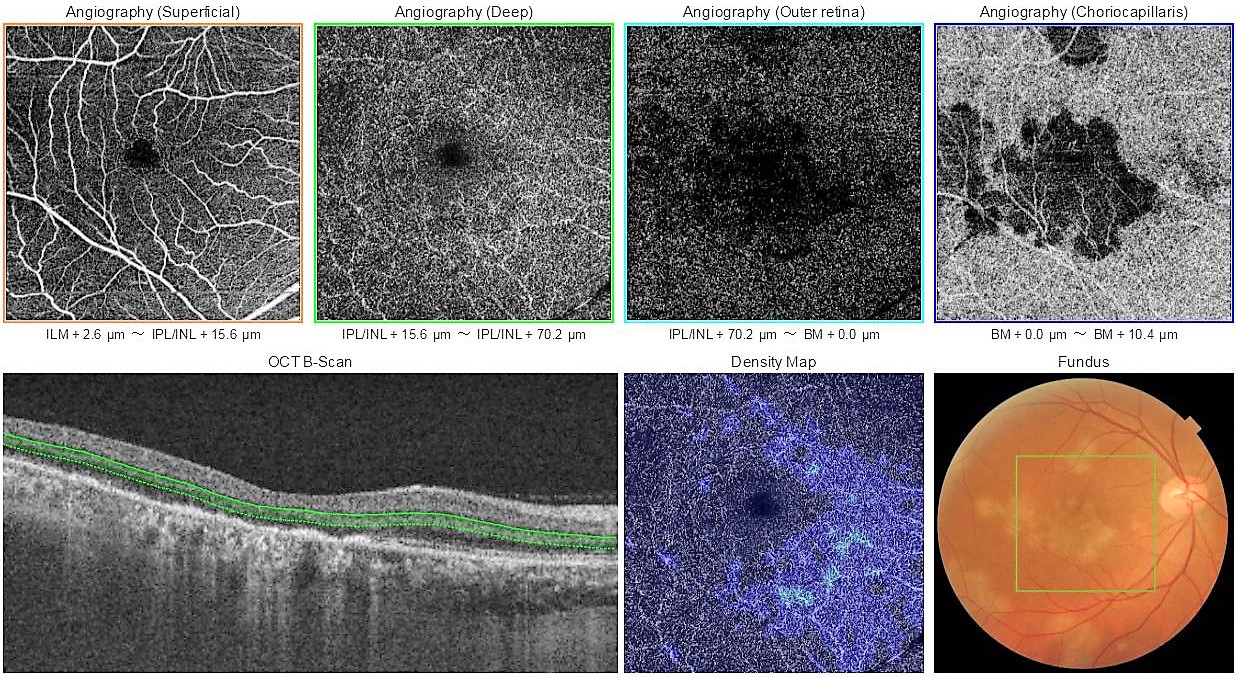
Figure 6. OCT angiography of the right eye of a patient with multifocal serpiginoid choroiditis, presumably due to TB, showing the vasculature (blood vessel network) in the deep retina and choroid. - B-Scan: This is a non-invasive scanning technique where a an ultrasound probe is placed on the closed eyelids of the patient. In uveitis, it is mainly used the study inflammation of the posterior sclera (white outer coat of the eye). (Figure 7).
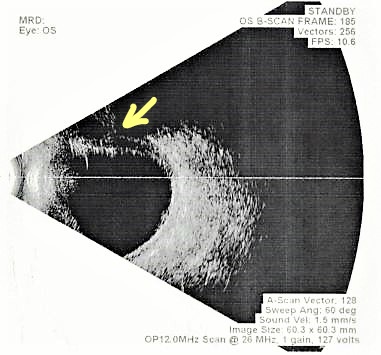
Figure 7. Ultrasound B-scan of a patient with scleritis (inflammation of the white portion of the eye) and superior exudative retinal detachment (arrow). - Ultrasound biomicroscopy (UBM): This is also a non-invasive scanning technique used mainly to study the anterior scleral lesions. (Figure 8).
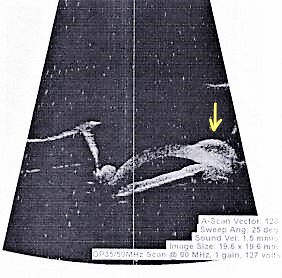
Figure 8. UBM scan of a patient with scleral abscess (arrow) due to tuberculosis - Visual fields: This is used to study optic nerve involvement due to disease or drug toxicity. (Figure 9)
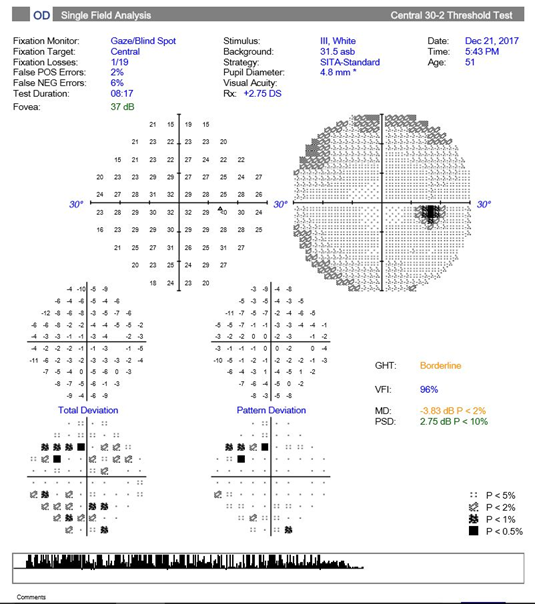
Figure 9. Visual fields report
- External eye photography (Figure 1)
-
-
Systemic investigation: We refer patients to an NABL accredited diagnostic laboratory for the following systemic tests:
- Mantoux test: It is a test of immunity to tuberculosis antigen. 0.1 ml 5 tuberculin units of purified protein derivative is injected into the skin of the forearm and reaction to it is measured after 48 hours. The test is considered positive (i.e. patient is likely to have latent / active tuberculosis) when the induration (skin swelling) is 10mm or more. At 10mm, the sensitivity (ability of the test to correctly identify those with the disease) of the test is 71% and specificity (ability of the test to correctly identify those without the disease) is 66%. In HIV positive patients >5 mm induration is considered a positive reaction. Mantoux test is cutaneous hypersensitivity to tuberculin antigen and it has been proven that cutaneous hypersensitivity correlates with ocular hypersensitivity. Thus this test is important in diagnosis of ocular disease.Sometimes, patients are told that a positive mantoux test has no meaning in our country because we all have taken BCG vaccination at birth. This does not hold true, as according to the recommendations of the Advisory Council for elimination of tuberculosis, Center for Disease Control and Prevention: Screening for tuberculosis infection in high-risk populations, the probability that the reaction in mantoux skin test is from the Mycobacterium tuberculosis antigen and not due to BCG increases:
- with increase in size of reaction,
- with a patient who has been in contact with a person who has TB,
- with family history of TB or patient’s country of origin has a high incidence or prevalence of TB, and
- with an increasing interval between vaccination and skin testing. Vaccination-induced reactions wane with time and are unlikely to persist for more than 10 years.
Also, even according the United States Preventive Services Task Force, any induration of more than 10 mm should not be attributed to prior BCG vaccination.
Recently, a new test, Quantiferon TB gold has been introduced for the detection of tuberculosis. This is a blood test that quantifies release of interferon gamma by stimulated sensitised T-cells in response to M. tuberculosis antigen ie. it measures release of a specific substance in the body in response to TB infection. Theoretically, it is not supposed to give false-positive results. However, about 41% healthcare workers and about 80.5% HIV positive patients with low-risk may show false-positive results. Like, Mantoux test it also does not differentiate between active and latent TB infection. According to the World Health Organization, “Latent Tuberculosis Infection: Updated and Consolidated Guidelines for Programmatic Management”, 2018, either a mantoux skin test or/ Quantiferon TB gold [interferon-gamma release assay (IGRA)] can be used to test for LTBI (strong recommendation, very low-quality evidence) and BCG vaccination should not be a determining factor in selecting a test. However, since there is no gold standard for testing for LTBI, we prefer, Mantoux test since it is cost effective and easily available.
- Mantoux test: It is a test of immunity to tuberculosis antigen. 0.1 ml 5 tuberculin units of purified protein derivative is injected into the skin of the forearm and reaction to it is measured after 48 hours. The test is considered positive (i.e. patient is likely to have latent / active tuberculosis) when the induration (skin swelling) is 10mm or more. At 10mm, the sensitivity (ability of the test to correctly identify those with the disease) of the test is 71% and specificity (ability of the test to correctly identify those without the disease) is 66%. In HIV positive patients >5 mm induration is considered a positive reaction. Mantoux test is cutaneous hypersensitivity to tuberculin antigen and it has been proven that cutaneous hypersensitivity correlates with ocular hypersensitivity. Thus this test is important in diagnosis of ocular disease.Sometimes, patients are told that a positive mantoux test has no meaning in our country because we all have taken BCG vaccination at birth. This does not hold true, as according to the recommendations of the Advisory Council for elimination of tuberculosis, Center for Disease Control and Prevention: Screening for tuberculosis infection in high-risk populations, the probability that the reaction in mantoux skin test is from the Mycobacterium tuberculosis antigen and not due to BCG increases:
-
Chest X-Ray / High-resolution Computed Tomography (HRCT) Chest:
Although traditionally chest X-ray is used for the diagnosis of pulmonary (lung) tuberculosis, it has been shown in a study published in 2014 in the International Journal of Infectious Diseases, that HRCT (high resolution CT scan of the lung) is better than chest X-ray in predicting lung TB, with a sensitivity of 96% versus 48%. A study published in the Turkish Thoracic Journal in 2016, supported the use of HRCT chest in the diagnosis of lung TB even in patients in whom the bacteria were not seen in the sputum test. In our study from Neoretina (Figure 10), we proved the utility of HRCT chest in the diagnosis of ocular tuberculosis even in patients who had a negative or inconclusive mantoux test. We concluded that HRCT has an important role in the accurate diagnosis of ocular tuberculosis, especially in the absence of other confirmatory tests. Correct diagnosis of this treatable condition is essential for the prevention of blindness from recurrent uveitis. This is also important to obviate the risk of reactivation of systemic tuberculosis from the use of steroid only therapy in this group of patients.
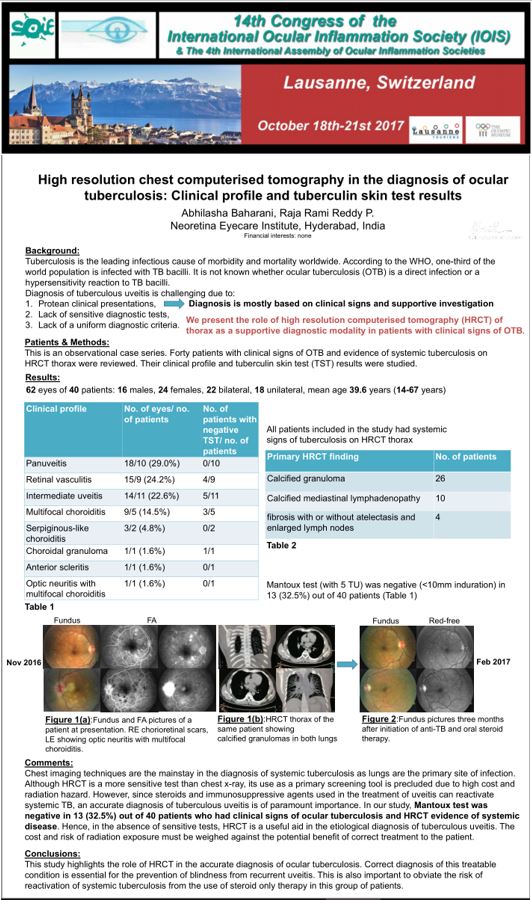
Figure 10. Our study presented at the Congress of the International Ocular inflammation Society, Lausanne, Switzerland, 2017.
What are the diagnostic categories of Ocular Tuberculosis?
At Neoretina, our treatment protocols are based on the latest Index-TB Guidelines, Guidelines on Extrapulmonary Tuberculosis in India, published by the Central TB Division, Ministry of Health and Family Welfare, Government of India in 2016. The following diagnostic categories have been defined:
- Possible ocular TB: Patients with the following (1, 2 and 3 together or 1 and 4) are diagnosed as having possible ocular TB:
- At least one clinical sign suggestive of ocular TB and other causes excluded.
- X-ray/CT chest not consistent with TB infection and no clinical evidence of extraocular TB
- At least one of the following:
i. Documented exposure to TB (family history of TB)
ii. Immunological evidence of TB infection (positive Mantoux or Quantiferon TB gold test) - Molecular evidence of Mycobacterium tuberculosis infection (confirmation through testing of fluid from the eye).
- Clinically diagnosed ocular TB: Patients with all the following (1, 2 and 3 together) are diagnosed as having probable ocular TB:
- At least one clinical sign suggestive of ocular TB, and other causes excluded
- Evidence of chest X-ray consistent with TB infection or clinical evidence of extraocular (outside the eye) TB or microbiological confirmation from sputum or extraocular sites
- Documented exposure to TB and/or immunological evidence of TB infection.
- Bacteriologically confirmed ocular TB: A patient with at least one clinical sign of ocular TB, along with microbiological (smear/culture) or histopathological confirmation of Mycobacterium tuberculosis bacteria from ocular fluids/tissues.
How is Ocular TB treated?
Patients in all the three described diagnostic categories are treated with anti-tubercular therapy (ATT) for at least 9 months. Longer duration of treatment is required for prevention of recurrences. During follow-up treatment is monitored by regular eye examination and eye scans, colour vision and liver function tests to look for any drug toxicity. Corticosteroids (local or systemic) and are used as adjunctive treatment for the control of inflammation. Locally steroids may be used as eyedrops, depot steroid near the outer coat of the eye (posterior subtenon injection) or as a low dose dexamethasone implant inside the eye (Ozurdex). We prefer local injections when the risk of systemic side effects of steroids are higher, like in pre-existing diabetes, hypertension (high BP), osteoporosis (weak bone structure) or when the disease is unilateral and systemic steroids use is not justified or when the patient is unable to tolerate systemic steroids.
How is response to treatment monitored?
Since microbiological confirmation might not be possible with ocular tissues, we monitor the response to treatment by the level of inflammation in the eye. Disease is said to be in remission when there is no inflammation for at least 3 months after completion of treatment. Relapse is when there is 2-step increase in inflammation after complete remission. Treatment failure is when there is no decrease in inflammation or less than 2-step decrease in inflammation after 3 months of ATT. In case of treatment failure, we look to rule out other causes of uveitis. Sometimes a paradoxical reaction (increase in inflammation to tuberculosis antigen) may occur, generally 2 months after starting ATT. In such cases steroid therapy needs to be stepped up. Lastly, we take fluid from the eye for molecular diagnosis of tuberculosis and to test for drug resistance.
Is surgery also required for the treatment of Ocular TB?
Surgery may also be required, usually when there are complications of uveitis such as:
-
- Neovascularization (growth of abnormal blood vessels in the retina which tend to bleed) in cases of retinal vasculitis (inflammation of retinal blood vessels). Such cases may be treated with retinal laser, which is an outpatient procedure. In case of non-resolving vitreous haemorrhage (bleeding inside the eye), a vitrectomy surgery (removal of the vitreous, the gel occupying the inside of the eye, where the bleeding has occurred) may be required.
- Persistent floaters after completion of treatment. In such cases also vitrectomy may help.
- Cataract: cataract surgery with intraocular lens implantation is done.
- Glaucoma: If medically uncontrolled, surgery may be required to control the intraocular pressure.
In summary, diagnosis of ocular tuberculosis is a difficult task but a keen clinical eye and a combination of diagnostic tools and methods help in the same. It is important for patients and clinicians to understand the diagnostic and treatment methods in order to remove the stigma and fear associated with this disease. Like in every other branch of medicine, an early, accurate diagnosis, and prompt and appropriate treatment is so critical in achieving favourable results. A systematic approach and proper diagnosis at the initial stages, before complications of the disease set in, helps to avoid inadvertent use of steroids with recurrence of tuberculosis uveitis and improves visual outcome of this sight-threatening disease several fold.
-

Ocular Tuberculosis Part 2: Frequently Asked Questions
Visit Our Previous Blog Ocular Tuberculosis Part 1
These are actual questions from patients in the Uvea Clinic of Neoretina.
-
Can TB affect the eye?
- Yes. TB (tuberculosis) can affect the eye, damage the delicate structures of the eye and cause loss of vision.
-
How did I get TB? Nobody in my family has TB.
- TB bacteria are released in the environment if a person with TB coughs or sneezes. Each such droplet containing millions of bacteria is suspended in the air for several minutes. If you inhale these droplets containing bacteria, you might get infected with TB. Only 10 bacteria are sufficient to cause infection.
-
Can I infect other members of my family if I have eye TB?
- Don’t worry, if you have TB only in the eye, you will not affect other members of your family. It is only when you have an active disease in the lung, can you infect others in the family.
-
Can I die from eye TB?
- No, you cannot die from eye TB. It is a treatable condition. Only, untreated, active and severe systemic TB can be fatal.
-
Doctor, what stage of TB do I have?
- There are no stages defined for ocular TB as such, but taking treatment early, i.e. before complications from the disease develop results in better visual outcomes.
-
Can I have a normal family life if I have been diagnosed with ocular TB?
- Yes, you can have a normal family life if you have only eye TB, but if you have active disease in the lung, you should take the following precautions:
- Keep your hand over your mouth when you cough or sneeze and keep washing your hands with soap and water.
- Stay in a separate well-ventilated room.
- Sleep in a separate room away from your family members.
- Avoid close contact with others.
- Do not go to work or school.
- Yes, you can have a normal family life if you have only eye TB, but if you have active disease in the lung, you should take the following precautions:
-
Will you be treating my eye TB at Neoretina or do I have to consult a physician?
- Yes, I will be treating you with the anti-TB treatment at Neoretina and also monitor the disease response and side effects of medication.
-
Will my lung TB also get cured if I take anti-TB course correctly?
- Yes, it will.
-
Is it a lifelong treatment?
- No, the treatment duration is only nine months.
-
Why have you prescribed so many tablets? Is one tablet not enough?
- TB treated with multiple drugs is more effective in killing the bacteria. Also, it helps avoid the development of multidrug-resistant TB (MDR-TB). This resistant form of TB is more difficult to treat.
-
Can I take the prescribed medicines throughout the day instead of morning?
- No. Prescribed medicines should be taken only in the morning as advised by the doctor. This helps the blood levels of the drugs to peak at the same time and hence, it is more effective in killing the bacteria.
-
Doctor, there are too many tablets, won’t it cause increased heat in the body?
- No, it doesn’t cause “increased body heat” or rise in body temperature. A doctor prescribes the medication only after checking your weight, so the dosage is in accordance with your weight.
-
What are the side effects that I may experience while on TB treatment?
- Your urine will be orange coloured, nothing to worry about. You might experience nausea, vomiting and reduced appetite in the initial period. However, if it is excessive, contact your doctor. At Neoretina, we monitor the side effects with regular colour vision and blood tests for liver enzymes. In case you develop raised liver enzymes, resulting in nausea and vomiting, your doctor will treat you with additional medication.
- Some patients may also develop a transient rash with itching. This can also be well managed with additional medication.
-
What are the foods to be taken or avoided during treatment?
- A patient can take his regular diet; however, it is better to avoid very spicy or fried foods as it may cause further acidity and gastritis. If you’re experiencing nausea, vomiting, and reduced appetite, take small frequent meals, do not lie down immediately after a meal, eat bananas, avoid gas forming/ processed foods and avoid eating sweets and creamy desserts. It is important to drink a lot of water (10-12 glasses per day) and keep yourself hydrated.
-
Will you do surgery for my eye TB or only tablets are enough?
- Generally, tablets are enough. Surgery is required in cases where complications develop. For instance: new vessel formation in the retina in cases of retinal blood vessel inflammation can cause bleeding in the eye. In such cases, if the bleeding does not resolve even after retinal laser, a vitrectomy surgery (removal of the blood surgically) is undertaken. If there is a cataract, cataract surgery will need to be done.
-
I’m not from Hyderabad, what if I miss an appointment?
- If you miss an appointment or get delayed by a few days, do not stop the medication. There is no harm in taking the medication for a few extra days, but discontinuation or missing the doses is not advisable.
-
Can I go to work while on treatment?
- Yes, you can if you have only eye TB because eye TB is not contagious.
-
Can I breastfeed while on treatment?
- Though anti-tuberculosis drugs get secreted in the milk, the quantity is very minimal and you can breastfeed while on treatment. But you must inform the doctor that you’re breastfeeding so she can add an adequate dose of Vitamin B6 to your regimen.
To continue reading on this subject, visit our next blog Ocular Tuberculosis Part 3
-
-

Ocular Tuberculosis Part 1: Clinical cases treated at Uvea Clinic, Neoretina
The term “Ocular Tuberculosis” is defined as an extra-pulmonary form of the disease that includes any infection in or around the eye caused due to Mycobacterium tuberculosis. It may be either active infection or an immunologic reaction, related to delayed hypersensitivity (an aseptic reaction to tubercular antigen).Ocular Tuberculosis is categorised into two types, in case of primary ocular TB: the eye is the initial port of entry into the body, and for secondary one, the infection spreads via the bloodstream from a distant site or a direct invasion from adjacent areas like the sinus or the cranial cavity.In Ocular Tuberculosis, every tissue of the eye can get affected. The patient suffering from Ocular TB , if untreated, usually runs a chronic course with exacerbations and remissions.
Following are a few cases that have been treated at Uvea Clinic, Neoretina:
Case 1. A 55 year old lady presented with sudden loss of vision in her left eye since 10 days. On examination her left eye showed swelling of the optic nerve with swelling and whitening of the adjacent retina and multiple foci of choroiditis (inflammation of the choroid). Her mantoux test was positive and her HRCT chest showed evidence of old tuberculosis infection. She was treated with anti-TB therapy for 9 months and her vision completely recovered, without any scarring or visual field loss. Therefore timely diagnosis and treatment can lead to excellent results.
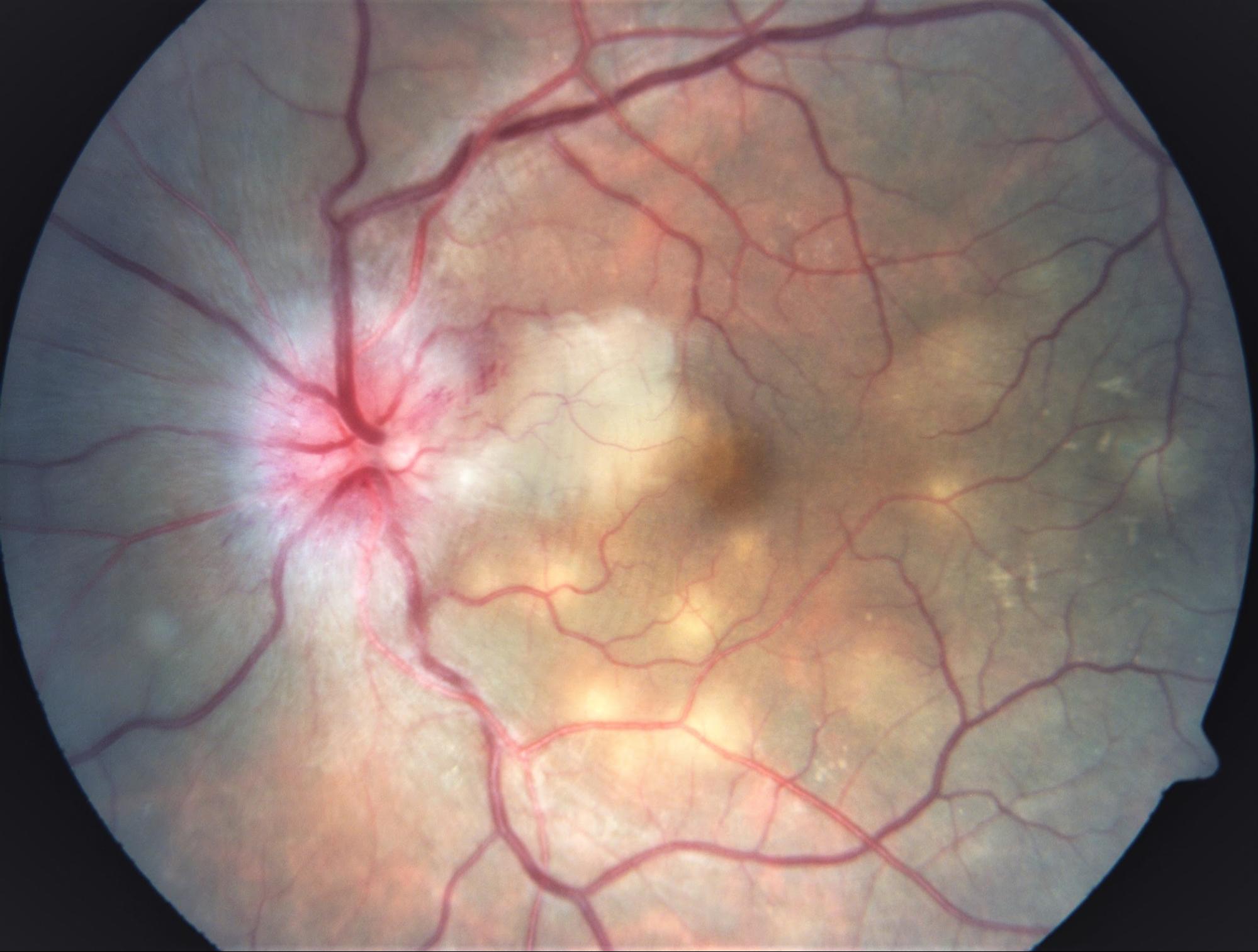
Neuroretinitis with choroiditis. Visual acuity : counting fingers at 2 metres
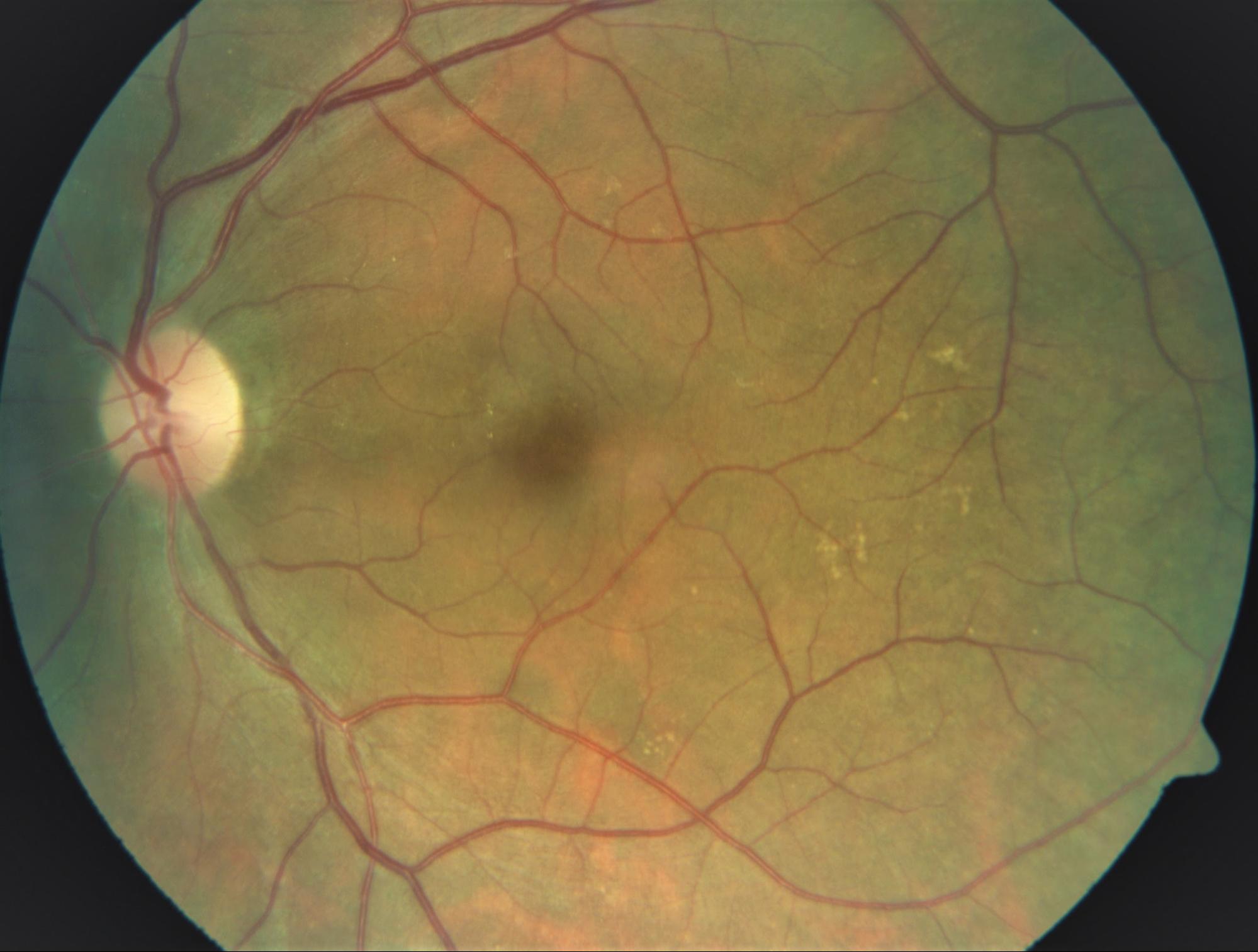
After 2 months of treatment. Visual acuity: 6/6
Case 2. A 47 year old gentleman presented with decreased vision in his right eye since more than 10 years but sudden loss of vision since 2 days. He had been treated several times for his eye problem with multiple courses of steroids at various hospitals in the past. On examination his right eye showed extensive scarring of the retina with a active edge of choroiditis passing through the macula (central, sensitive portion of the retina). His mantoux test was negative but HRCT chest showed evidence of tuberculosis. Hence he was treated with 9 month course of anti-TB therapy and his vision recovered completely, although with extensive scarring and visual field loss. In this patient because of delay in presentation, inappropriate treatment with steroids, there was extensive scarring of the retina, which could not be reversed even with treatment. However, patient recovered 100% visual acuity and further damage was prevented. It is therefore important to get the right treatment before complications of the disease develop.
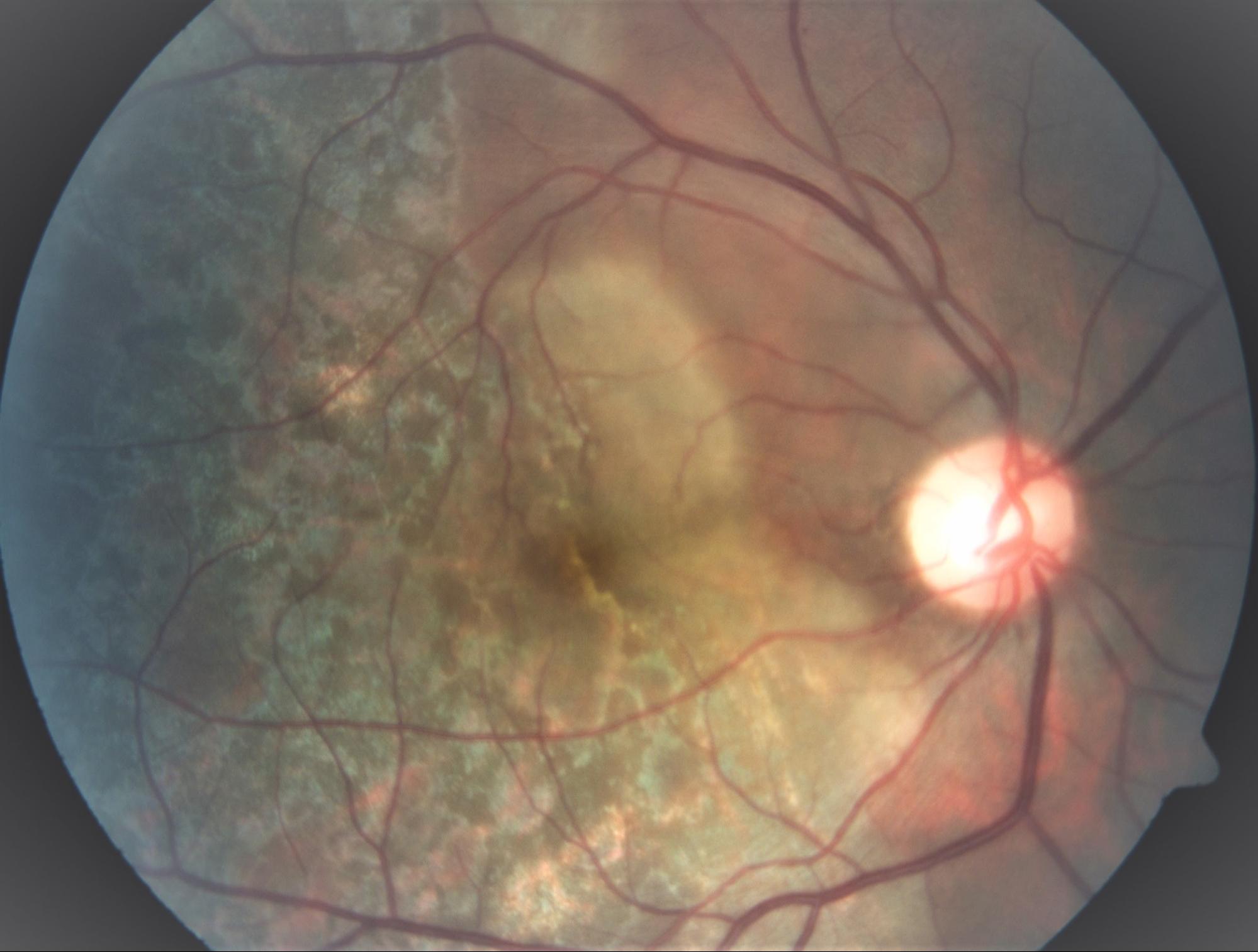
Extensive choroiditis with active edge. Visual acuity: hand movements
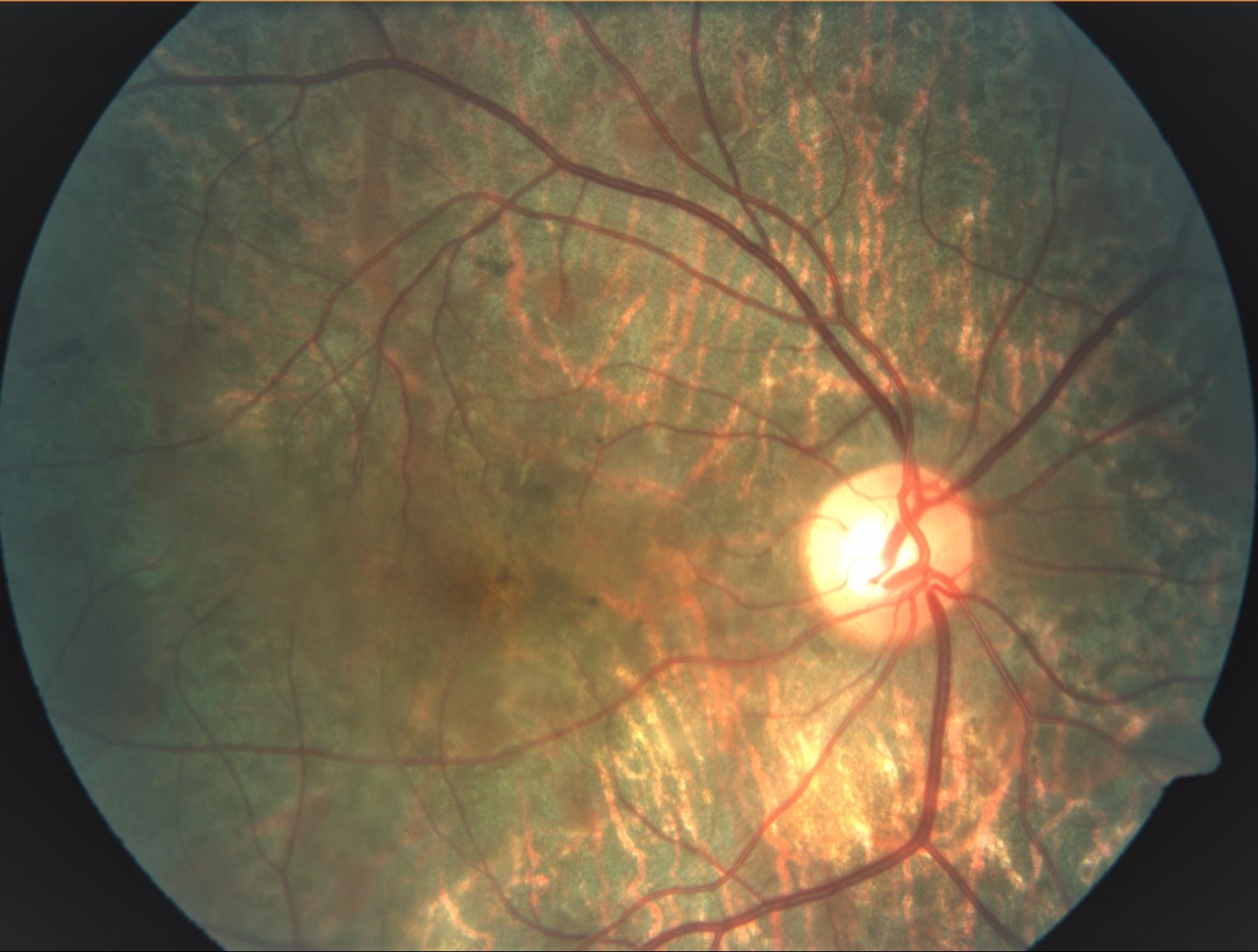
After 5 months of treatment. Extensive scarring, though visual acuity 6/6
Case 3. A 28 year old gentleman presented with severe redness, pain and reduced vision in his left eye since 15 days. He was being treated elsewhere with steroid eyedrops but to no avail. On examination his left eye showed inflammation of the sclera (white outer coat of the eye) with whitening in the adjacent cornea (transparent front portion of the eyeball, important for clear vision). He also had inflammation of the vitreous cavity (inner gel of the eye) and cystoid macular oedema (swelling of the centre of the retina). He complained of pain in the abdomen, radiating to the back since 1 year. His mantoux test was positive and guided by his abdominal symptoms we did an HRCT of the abdomen which showed multiple enlarged calcified lymph nodes and active TB with strictures in his kidney. We immediately started him on anti-TB treatment and referred him to the nephrologist. They agreed with our diagnosis and treated his kidney strictures with stent. He was relieved of his eye and abdominal symptoms in 3 weeks and his eye and kidney TB recovered fully with treatment. Timely diagnosis and treatment of TB is not only sight saving, it can also be life-saving.

(Top) Sclerokeratitis (inflammation of the sclera and cornea) with (bottom) intermediate uveitis and cystoid macular oedema.

After 6 months of treatment. Completely resolved sclerokeratitis (Top) and cystoid macular oedema (bottom)
Ocular Tuberculosis cases highlight the fact that manifestations and clinical symptoms of the infection can differ drastically in patients. Hence, it needs a thorough examination, prompt diagnosis, and timely treatment. Early diagnosis and quick therapy can help in preventing further complications. Clinicians and ophthalmologists should be aware of such cases and findings when treating patients with this vision-threatening disease and patients with tuberculosis uveitis shouldn’t lose hope.
To continue reading on this subject, visit our next blog Ocular Tuberculosis Part 2
-

Glaucoma: Symptoms, Prevention, and Treatment
The Optic Nerve, also known as the ‘second cranial nerve’ is responsible for transmitting visual information from the eye (retina) through electrical impulses to the vision centers of the brain. (more…)
-

Focal Laser: Indications and Treatment
Focal laser is explained as a photocoagulation procedure wherein the laser is applied to vascular abnormalities and or leaking areas in the retina especially in the macular area (more…)
-

Neoretina gets NABH Accreditation
A clear sight is a blessing in this world. This does not mean just how far one can see but also how sharp one can see. There is a reason that peripheral vision assumes so much significance for human beings.
-

Diabetic Retinopathy (DR): Symptoms and Treatment
The retina is a light-sensitive layer lining the inside of the eye capturing the light travelling through the eye. Diabetes mellitus (a disease with deranged sugar metabolism) over a period of time affects the eye.
-

Symptoms, Causes and Treatment of Uveitis
Uveitis is one of the leading causes of irreversible blindness. The problem is rampant in developing countries like India. It becomes important for the patients and their relatives to know what Uveitis is and what they can really do about it.